The Real Reason Men Over 50 Lose Their Erections Has Finally Been Identified — And It Is Not What Your GP Told You

If you are a man over 50 who still feels desire but whose body no longer responds the way it should — read every word of this page.
This is not about pills. Not about pumps. Not about anything you have tried before.
You Know Exactly What This Feels Like
There is a moment every man recognises.
You are in bed with your wife. Or someone you have been seeing. The mood is right. You want this — part of you has been thinking about it all day, maybe all week. The desire is real and present and completely intact.

And then nothing.
Or almost nothing.
Something that starts and fades before it fully arrives.
Something that used to be automatic, effortless, reliable — and now feels like trying to start a car on a February morning that may or may not turn over.
And in those ten or fifteen seconds, something happens inside you that has nothing to do with sex.
You feel shame.

Not the dramatic, spoken kind.
The quiet kind.
The kind that settles in your chest without announcement and stays there.
The kind that doesn’t get discussed — not with your GP, not with your mates down the pub, and certainly not with her.
Because men of your generation were raised not to say these things.
You were raised to manage. To get on with it. To not make a fuss.

So you make a joke. Or you say you’re tired.
Or you roll over and lie in the dark listening to her breathing slow into sleep while you stare at the ceiling and think about things you’d rather not think about.
And the next morning you’re perfectly fine.
You get up, you make tea, you go about your life the way you always have.
Strong. Capable. Reliable.
But somewhere underneath all of that — quiet and persistent — is the knowledge that something has changed. Something you cannot name precisely. Something you don't know how to fix.
Maybe you've noticed other things, too.
Morning erections — which used to be so reliable they woke you before the alarm — have become infrequent.
Or they’ve disappeared entirely. You never used to think about them.
Now you notice their absence the way you notice the absence of something that used to just be there.
You’ve started making small adjustments.
A weekend away that you’d have looked forward to now carries a quiet undercurrent of dread.
What if it happens again.
What if it doesn’t happen, rather.
You love your wife.
You find her attractive.
But somewhere in the last year or two you’ve started engineering reasons to go to sleep before her.
To be tired.
To be on your phone a little too long.
And she hasn’t said anything — because she’s perceptive and she’s kind and she doesn’t want to make it worse — but she’s noticed.
You know she’s noticed.

You have, perhaps, looked at the medication.
You might have even tried it. It works, technically.
But there’s something about it that sits uncomfortably.
The idea that the man you’ve spent fifty-odd years building now requires a tablet to perform a function that used to need nothing at all.
And the side effects don’t help — the headache behind the eyes, the face that flushes red at dinner, the way your heart feels like it’s working a little too hard.
These are not the conditions under which confidence returns.
So you manage. You adapt.
You carry it, the way you carry most things — quietly, and alone.


Here is what I want you to understand before you read another word of this page:
This is not age. Not inevitable decline. Not weakness, physical or mental. And it is almost certainly not what your GP suggested — a vascular issue, a blood pressure problem, a testosterone dip that a patch or a pill might address.
There is a specific, identifiable, biological reason this is happening to you. It has a name. It has a mechanism that has been studied and documented. And — critically — there is now a solution that addresses that mechanism directly, without pharmaceuticals, without side effects, and without any of the compromises you’ve been living with.
Keep reading.
The Part of Your Body Nobody Told You About
Most men — and, frankly, most GPs — think about erectile dysfunction in terms of blood flow.
The arteries narrow. The circulation slows. The blood doesn’t reach the tissue.
Take something to dilate the vessels and the problem is addressed.
For some men, that is accurate.
But for the majority of men over 50 who experience progressive erectile dysfunction — the kind that develops gradually over years, worsening slowly, becoming harder to explain away — the primary cause is something different.
Something deeper. Something that medication cannot reach.
It begins with a network of nerve fibres that most men have never heard of — and that most doctors never mention.
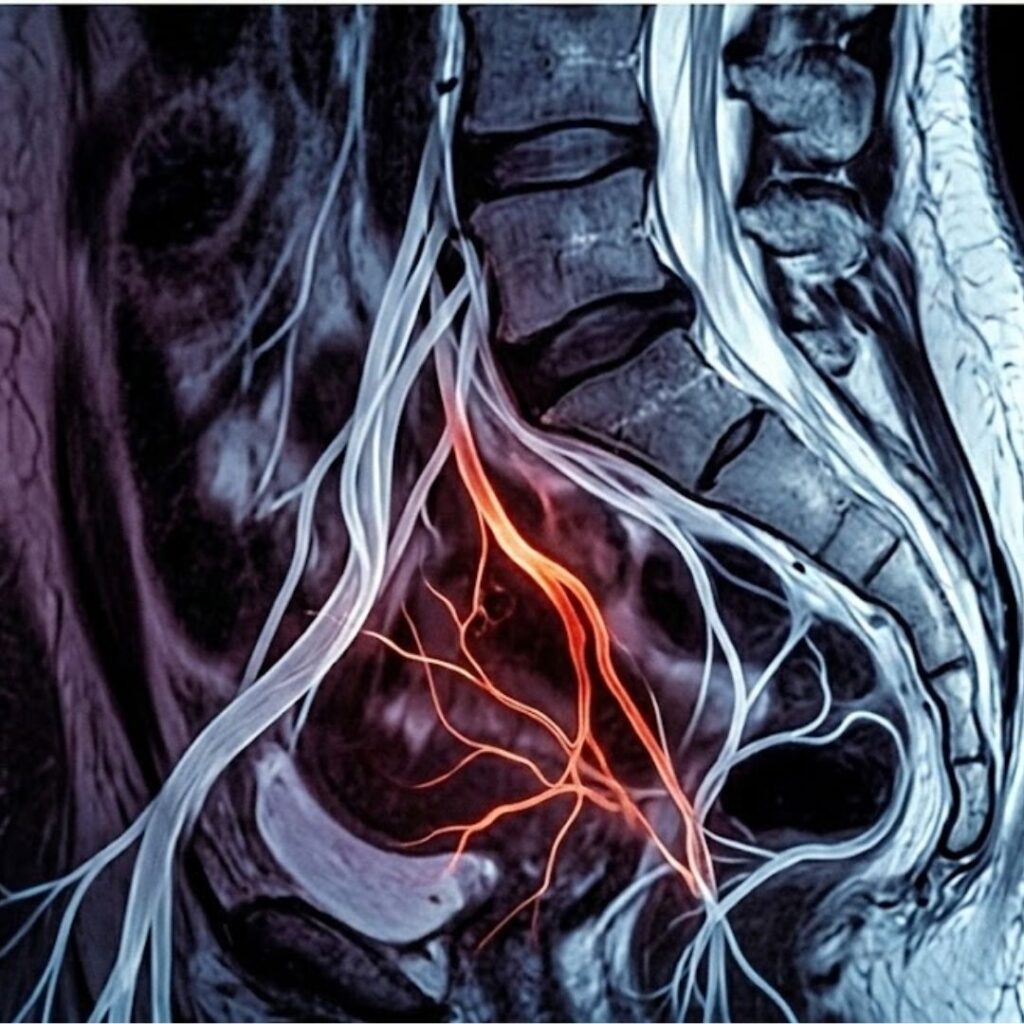
The Cavernous Nerves — The Wiring Behind Every Erection

Running from the base of your spinal cord, through your pelvic region, and into the erectile tissue of the penis, there is a set of nerve fibres called the cavernous nerves.
These nerves are part of the autonomic nervous system.
They operate entirely below the level of conscious control.
You have never had to think about them. They simply do their job.
Here is what that job is:
When your brain registers arousal — a thought, a touch, a visual stimulus, an emotional connection with someone you love — it generates an electrical signal.
That signal travels down through the spinal cord, passes through a nerve relay point in the pelvis called the pelvic plexus, and then travels along the cavernous nerves directly into the smooth muscle tissue lining the corpora cavernosa — the two chambers inside the penis that fill with blood during erection.
The signal instructs that smooth muscle to relax.
When the muscle relaxes, the internal blood vessels dilate. Blood rushes into the chambers. The penis becomes erect.
That is the entire system. Brain generates signal. Cavernous nerves carry it. Smooth muscle relaxes. Blood fills the chambers. Erection occurs.
Elegant. Automatic. It has been working without any conscious effort on your part since adolescence.
Until, gradually, it stopped.
What Happens When the Wiring Degrades
Think of a copper cable running between a light switch on one side of a room and a lamp on the other.
When the cable is intact and its insulation is healthy, you flick the switch and the lamp lights immediately.
The signal travels cleanly, at full strength, with no loss.
Now imagine that the insulating layer around the cable has been slowly, invisibly degrading for fifteen or twenty years.
Not snapped.
Not visibly broken.

But the protective coating has been wearing away — millimetre by millimetre, year by year — until the copper inside is exposed in places, and the signal that travels along it begins to lose coherence.
One day you flick the switch and the lamp flickers.
Then it takes a moment to come on.
Then it comes on dimly.
Then there are days when it doesn’t come on at all.
The switch is fine.
The lamp is fine.
The problem is in the cable.

This is what happens in the cavernous nerve network of the majority of men who develop progressive erectile dysfunction after the age of 50:
The protective myelin sheath that insulates the cavernous nerve fibres begins to degrade.
This process — called progressive cavernous nerve demyelination — is silent, cumulative, and slow.
Most men don’t notice it until the damage has already become significant, because the nervous system compensates for minor degradation in ways that aren’t obviously detectable.
The brain continues to generate the arousal signal perfectly.
The desire is completely intact.
But the signal travels along a compromised nerve pathway — losing strength, losing speed, losing precision with every millimetre of degraded myelin it passes through — and arrives at the smooth muscle tissue too weakened to trigger the full relaxation response.
The blood doesn’t rush in the way it once did.
The erection is partial. Or slow. Or it starts and then fades before it’s fully there.
It is not that your body does not want to respond. It is that the message is no longer getting through cleanly. And every month that passes without addressing the underlying nerve degradation, a little more of the signal is lost in transit.

This is also why medication becomes progressively less effective for so many men over time.
Drugs like sildenafil and tadalafil work by amplifying the vascular response — they force the blood vessels to dilate more aggressively, compensating for the weakened nerve signal.
For a while, this works. But as the nerve pathway continues to degrade, even the pharmacologically amplified response can no longer compensate.
The doses stop being effective. The windows of effectiveness shorten.
You are not failing the medication.
The medication was never treating your actual problem.
The only genuine solution for progressive cavernous nerve demyelination is to address the nerve pathway itself — to restore the wiring, not to turn up the volume at the lamp end of a fraying cable.
For years, there was no way to do this outside a clinical setting. That changed in Bristol, three years ago.
Why This Is Happening — The Four Causes Nobody Connected
Before we come to what changed in Bristol, it is worth understanding how cavernous nerve demyelination happens in the first place.
Because it does not happen randomly. There are four specific, documented causes — and every man reading this will recognise at least two of them in his own history.
1. Alcohol — The Nerve Toxin Nobody Mentions

Ethanol is directly neurotoxic.
This is not contested in pharmacology.
It is documented, published, and almost never discussed in the context of sexual health.
Alcohol causes progressive damage to peripheral nerve fibres throughout the body via two mechanisms.
First, ethanol and its metabolites directly attack the myelin sheath, the protective insulating coating that keeps nerve signals clean and strong.
Second, chronic alcohol consumption depletes the body’s stores of B vitamins — particularly B1 (thiamine) and B12 — which are essential for myelin maintenance and repair.
Without adequate B12, the body cannot rebuild myelin fast enough to keep pace with alcohol-induced degradation.
The cavernous nerves are peripheral autonomic fibres.
They are among the most vulnerable nerve structures in the body to alcohol-related demyelination — partly due to their anatomical position, and partly because the myelin around autonomic nerve fibres is naturally thinner than the myelin around motor nerves and therefore degrades faster under sustained chemical stress.
Research published in the European Journal of Neurology found measurable reductions in penile nerve conduction velocity — a direct measure of cavernous nerve signal strength — in men consuming as few as fourteen units of alcohol per week over a period of ten years or more.
Fourteen units. That is two medium glasses of wine each evening. Perfectly ordinary. Socially invisible. Never discussed in the context of what has been happening in your bedroom.
The damage accumulates silently.
And it continues even after drinking stops — because the myelin that has already degraded does not repair itself without specific intervention.
2. Tobacco — Starving Your Nerves One Year at a Time

The cavernous nerve fibres require a continuous, reliable supply of oxygenated blood to maintain healthy myelin.
They are living tissue.
They have metabolic needs.
And tobacco smoke is systematically depriving them.
Smoking causes progressive vasoconstriction — narrowing — of the microvascular network.
The tiny blood vessels that supply oxygen and nutrients to peripheral nerve tissue contract under the sustained chemical influence of nicotine and tobacco combustion byproducts.
Over years of smoking, these vessels become chronically narrowed.
The nerve fibres they supply are slowly starved of the oxygen they need to maintain their myelin.
Myelin that is chronically oxygen-deprived begins to thin.
Thin myelin conducts electrical signals poorly.
Poor conduction means weaker signals reaching the smooth muscle tissue.
Weaker signals produce weaker, less reliable erections.
What most men do not realise — and what is almost never mentioned in smoking cessation campaigns — is that the peripheral nerve damage from long-term tobacco use does not reverse when the cigarettes stop.
The blood vessels recover.
The lungs begin to heal.
But the myelin damage that has accumulated in peripheral nerve fibres over years of oxygen deprivation does not simply undo itself.
If you smoked for ten, fifteen, or twenty years — even if you gave up a decade ago and are rightly proud of having done so — the cavernous nerve degradation from those years may still be active and progressive today.
3. Prostate — The Anatomical Problem
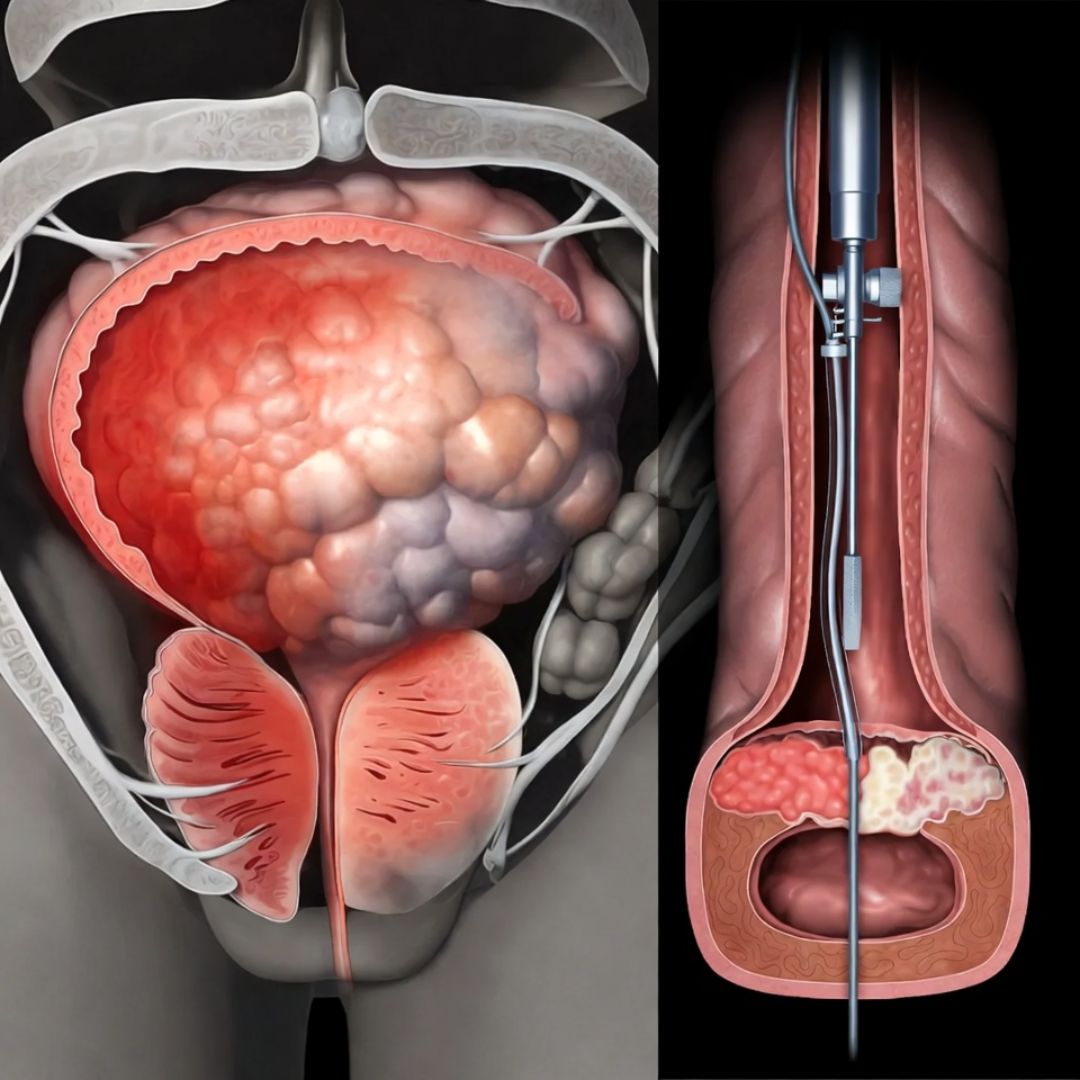
The cavernous nerves do not travel through the body in isolation.
They pass in close anatomical proximity to the prostate gland — running alongside it on either side as they make their way from the pelvic plexus to the erectile tissue.
This proximity creates a vulnerability that most men are never told about.
Chronic prostatitis — inflammation of the prostate — is one of the most underdiagnosed conditions in men over 45.
Studies suggest that as many as one in three men in this age group experience subclinical prostate inflammation: inflammation that causes no obvious pain, no urinary symptoms, nothing that would send a man to his GP — but which is detectable on imaging and measurable through inflammatory biomarkers.
Sustained prostate inflammation causes swelling in the tissue immediately surrounding the cavernous nerve bundles.
That swelling creates chronic pressure on the nerves — not acutely painful, but sufficient, over months and years, to cause compression-related damage to the myelin sheath.
The signal that passes through a compressed, inflamed nerve pathway degrades faster than it repairs.
For men who have undergone prostate surgery — whether for benign prostatic hyperplasia or for cancer — the situation is more direct.
The cavernous nerves are frequently damaged during prostatic procedures, sometimes unavoidably given their anatomical position.
Post-surgical erectile dysfunction is one of the most commonly reported consequences of prostate surgery in the UK, affecting tens of thousands of men every year.
Many are told to wait and see. Most find that waiting alone is insufficient.
4. Chronic Stress — The Parasympathetic Shutdown

This is the most misunderstood cause of all — and the one that is most frequently dismissed as psychological.
Erection is governed by the parasympathetic nervous system. It is fundamentally a rest-and-restore function.
For the physiological cascade of arousal to proceed — for the cavernous nerve signal to fire correctly and for the smooth muscle to respond — the body must be, at a neurological level, in a state of sufficient safety and relaxation.
Chronic stress does the opposite.
It activates the sympathetic nervous system — the fight-or-flight system — and in doing so actively suppresses parasympathetic function.
The cavernous nerve signals that should trigger erection are overridden by competing sympathetic activity.
This is the ‘psychological’ component of stress-related ED. It is real.
But it is physiological, not imaginary.
What is less commonly discussed is the long-term structural consequence of sustained sympathetic dominance.
Cortisol — the body’s primary stress hormone — at chronically elevated levels promotes a low-grade systemic inflammatory state.
That inflammation attacks myelin.
The same protective sheath that alcohol and tobacco degrade through different mechanisms is also degraded, more slowly but just as surely, by years of cortisol-driven inflammation.
Men who have spent their forties and early fifties running businesses, managing demanding careers, carrying the financial and emotional weight of families — men who have lived, in other words, the kind of life that is outwardly successful and inwardly exhausting — have often spent a decade or more with elevated cortisol.
The cavernous nerve degradation that results does not reverse when the stress eventually reduces. It stays. It compounds.
If you have recognised yourself in any of these four causes — and most men reading this will recognise themselves in at least two, often three — then what you are experiencing is not mystery and not decline. It is a physiological consequence of a specific, identifiable biological process.
And there is now a way to address it directly.
The Bristol Discovery — How a Rugby Study Changed Everything
Dr. Richard Harlow was not looking for this.
In the autumn of 2018, he was reviewing early data from a study he had been running for seven months at the University of Bristol’s Neural Repair Laboratory.
The study was funded by the Medical Research Council.
Its subject was peripheral nerve regeneration in former professional rugby players — men in their forties and fifties who had sustained chronic compression and impact damage to the peripheral nerve fibres of the lower limbs during years of professional play.
Many of these men had lived for years with persistent numbness, reduced sensation, and weakness in their legs and feet — damage that had been managed but never meaningfully reversed.
The working assumption in clinical practice was that peripheral nerve damage of this kind, once established, was essentially permanent.
Dr. Harlow's team were testing a different hypothesis.

They were working with a protocol based on low-intensity acoustic frequency therapy — precisely calibrated sound wave pulses delivered directly to the damaged nerve tissue.
The principle, borrowed from frontier research in sports rehabilitation medicine, was that specific acoustic frequencies could stimulate mitochondrial activity in the cells surrounding damaged nerve fibres.
And that by restarting mitochondrial energy production in those cells, you could provide the biological fuel needed for myelin repair to begin.
The hypothesis, stated plainly: you cannot force nerve regeneration from outside.
But you can restart the internal cellular engine that powers it.

By month seven, the data was quietly encouraging.
Several participants were showing measurable improvements in nerve conduction velocity in the treated limbs.
One man who had been unable to reliably feel the floor beneath his left foot for nearly four years told the research team, at his follow-up interview, that sensation had begun to return.
He cried during that interview.
Dr. Harlow noted it in the study log.
The results were solid. Modest.
The kind of progress that a careful researcher finds satisfying without finding exciting.

In November of that year, Dr. Harlow was twenty minutes into a standard follow-up interview with a 54-year-old former prop forward from Cardiff when the man paused, looked at the table between them, and said something quietly:
"I don't know if this is relevant to your study. Probably isn't. But — things have been different at home. With my wife. For the first time in about three years. I haven't told her yet because I didn't want to raise her hopes and then have it stop. But I thought you should know. In case it means something."